Endoscopic submucosal dissection of a lesion affecting the appendiceal orifice after appendectomy
Pedro André Lima1, André Mascarenhas1, Pedro Barreiro1,2, Cristina Chagas1
1 Serviço de Gastrenterologia, ULS Lisboa Ocidental; 2 Centro de Endoscopia Avançada de Lisboa, Hospital dos Lusíadas de Lisboa
DESCRIPTION
A 73-year-old woman underwent a colonoscopy, having been diagnosed in the cecum, centered on the appendiceal orifice, sessile polypoid lesion measuring approximately 25 mm, without endoscopic visible features of invasion (JNET2B classification). Given the location, it was proposed to appendectomy without evidence of neoplastic tissue in surgical specimen. A new colonoscopy was performed which confirmed the persistence of the lesion previously described in the appendicular orifice.
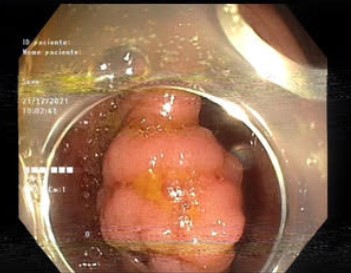 Figure 1. Sessile polypoid lesion in the appendicular orifice (after appendectomy).
Figure 1. Sessile polypoid lesion in the appendicular orifice (after appendectomy).
Given the location of the lesion (reaching the appendicular orifice/site of previous appendectomy – type 3a in the Toyonaga classification), predictable fibrosis, morphological pattern and dimension was proposed to endoscopic submucosal dissection (ESD). The procedure was performed with anesthetic support, Flush Knife 1.5 mm and with the aid of a traction method, lasting 75 minutes. The lesion was elevated followed by an incision in the mucosa and dissection of the submucosa with the help of clips and rubber band traction method. An en bloc resection without complications was achieved, highlighting the identification of the appendicular orifice during dissection, associated with severe fibrosis. The location corresponding to the appendicular orifice was closed with clips prophylactically.
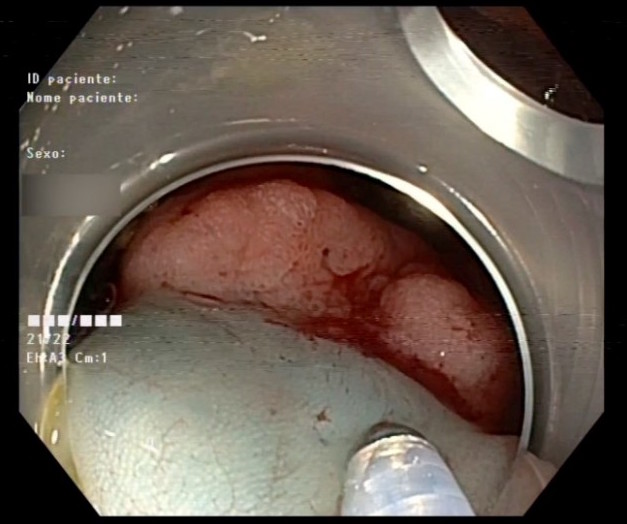 Figure 2. Endoscopic submucosal dissection.
Figure 2. Endoscopic submucosal dissection.
The pathological evaluation revealed that it was a tubular adenoma with low-grade dysplasia, focally with a lateral margin < 1 mm (HMx). Endoscopic reassessment was performed after 3 months without evidence of residual lesion. Stands out, however, invagination of the hem-o-lok® associated with previously placed clips, without evidence of perforation. Given that it was in the lumen of the colon, extraction was performed with biopsies forceps.
 Figure 3. Clips previously placed and Hem-o-lok®
Figure 3. Clips previously placed and Hem-o-lok®
DISCUSSION
Endoscopic submucosal dissection is used in specialized centers for the treatment of superficial neoplasia. Initially, it was considered that superficial neoplasia reaching of the appendicular orifice (L-PAO) could not be candidates for this technique given that it is a challenging anatomical design with a higher risk of incomplete resection and a higher risk of complications, namely perforation and/or acute post-procedure appendicitis1. However, recent work show promising results of this technique in this same location2.
In these lesions, it seems to be particularly useful to use the Toyonaga classification, in order to stratify the risk of incomplete resection and adverse events2. Recent work points to a technical success rate of endoscopic dissection in L-PAO greater than 90%, allowing avoid surgical treatment and its associated costs and morbidity. The traction method clips and rubber band, used in this case, may help en bloc resection2.
Lesions with deep invasion of the appendiceal orifice in patients without previous appendectomy (type 3) present a greater risk of perforations and difficulty in R0 resection. Approximately 25% of patients will require surgery to treat an urgent complication or incomplete resection. In these lesions, endoscopic full thickness resection would be a possibility, however, it is important to highlight the risk of acute appendicitis which can reach 25%. It should be noted that in lesions that extend from the appendix to the cecum, appendectomy may not be sufficient to treat the lesion. In patients undergoing appendectomy (type 3a), despite fibrosis, the procedure has greater probability of technical success and is associated with fewer complications compared to type 32 lesions.
REFERENCES
1. Jacob H, Toyonaga T, Ohara Y, et al. Endoscopic submucosal dissection of cecal lesions in proximity to the appendiceal orifice. Endoscopy. 2016;48(9),829–836.
2. Oung B, Rivory J, Chabrun E, et al. ESD with double clips and rubber band traction of neoplastic lesions developed in the appendiceal orifice is effective and safe. Endoscopy international open. 2020;8(3),E388–E395